
Some of the reasons to remove a tooth may be:
Impacted or mal-aligned teeth that may lead to problems in the future
Weakened, dead or symptomatic teeth
Failed root filling or extensive decay
Teeth affected by gum and bone disease
Prevention of complications such as infections
Removal of a retained root fragment of a tooth
Part of orthodontic treatment to create space for the orthodontist to align the teeth or to improve appearance of a smile
Removal of an extra (supernumary tooth)
Removal of a tooth that no longer has function
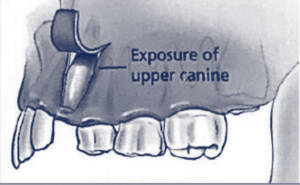
Unerupted teeth may become impacted and may require surgical exposure to help them erupt. Occasionally attachment of an orthodontic bracket may also be required to allow traction to be placed on the tooth to help erupt it.
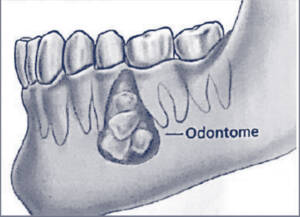
An odontoma is a primitive and malformed tooth. It can cause swellings, delay eruption or displace or affect the roots of adjacent teeth. An odontome should be removed whenever practicable.
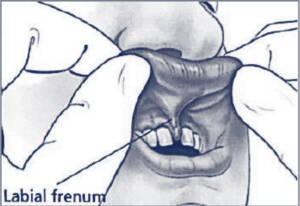
The upper lip is attached to the gums by a thin band of tissue called a “labial freenum”. Occasionally the freenum can be abnormally thick and cause a large gap between the front teeth.
The tongue is attached to the gums by a similar band of tissue called a “lingual freenum”. Occasionally this can limit movement of the tongue, swallowing or speech.
Removal of the freenum is called a frenectomy.
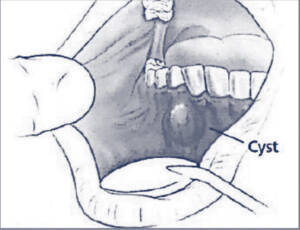
Cysts are fluid filled sacs that are slowly growing and can result in infection, pain and swelling. They can become large enough to affect nearby healthy teeth or strength of the jaws. Once diagnosed, they are best treated before symptoms arise or get worse. A tooth associated with the cyst may also need to be removed. Cysts can be treated by removal (enucleation) or opened with part of the lining removed (marsupialised).
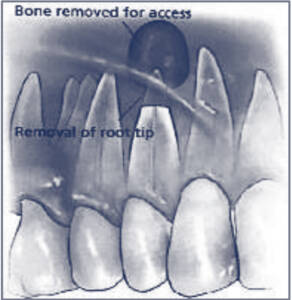
When a nerve and pulp tissue in a tooth dies, an abscess results at the tip of the root. An abscess can spread through the jawbone and cause severe illness. Surgery to remove the root tip, called an apicectomy, can clear the infection and potentially save the tooth. This needs to be done in conjunction with a root canal therapy performed by a dentist or endodontist.
A comfortable and functional fit for dentures may sometimes require surgery on the dento-alveolar ridges. The aim of surgery is to remove excessive gum tissues, fibrous tissues, scars or a bony outgrowth (“torus”).

For any abnormal tissue in the mouth, the entire tissue or a small piece may need to be removed for assessment. This is called a biopsy. The biopsy specimen will be sent to a pathologist to assess whether it is non-cancerous (benign) or cancer (malignant). The pathologist will send a report to your surgeon, who will subsequently discuss this with you. Occasionally a second biopsy may be needed if the first biopsy has an uncertain result.
